
Building on the findings that there is substantial variability and heterogeneity in the experience of suicidal thoughts, we sought to see if there was order to this heterogeneity. To do this, we applied to our two real-time monitoring studies a digital phenotyping approach, which refers to analyses (e.g., latent profile analysis, latent cluster analysis) that use multiple indices of data collected from a digital device (e.g., smartphone or wearable device) to identify profiles or phenotypes across people.
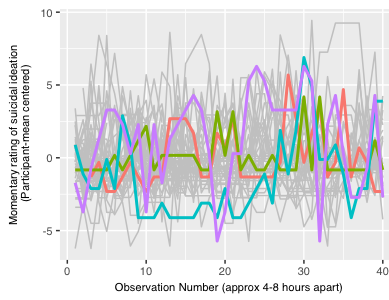
Using latent profile analysis (a type of analysis that creates groups or “profiles” of people a based on their responses to a set of variables), we found across both studies five distinct subtypes of suicide ideation (see figure to the left): (1) low mean, low variability (shown in green), (2) low mean, high variability (shown in yellow), (3) moderate mean and variability (purple), (4) high mean, low variability (red), and (5) high mean, high variability (blue). The phenotypes differ primarily in the average severity of suicidal ideation across measurement occasions, and the magnitude of within-person variability around that average. Moreover, the phenotype typified by more severe (i.e., higher mean) and more stable (i.e., lower within-person root mean square of successive differences [RMSSD]) suicidal ideation contained the highest proportion of individuals who had recently attempted suicide.
This is particularly interesting because it might mean that in the time immediately after a suicide attempt, people tend to have persistently high levels of suicidal ideation and as time passes, the mean level of ideation stays high and variability around that mean increases. This would assume that phenotypes are not static, and that people may shift from one phenotype to another in relationship to their environmental context (e.g., time since a suicide attempt, occurrence of life events).